




ABSTRACT
A case of unilateral coronoid hyperplasia successfully treated by corenoidotomy with prolonged postoperative physiotherapy and reveal the postoperative radiographic changes between the sectioned part of the coronoid process and the mandibular ascending ramus is described. The patient was a 28-year-old man whose maximum mouth opening was 30 mm. A coronoidotomy of the left coronoid process was performed. Nine days after surgery, the patient started physiotherapy with a HU-OSr appliance. After coronoidotomy and physiotherapy, the maximum mouth opening had increased to 43 mm. Radiographic follow-up showed that the coronoid process apparently united with the mandibular ascending ramus, with moderate dislocation and inclination posteriorly. In the case presented, an intraoral coronoidotomy with postoperative physiotherapy for treatment of coronoid process hyperplasia allowed satisfactory and stable results in the correction of coronoid-malar interference.
**********
In patients with coronoid process hyperplasia, which presents essentially a mechanical problem such as limited mouth opening, a surgical treatment with prolonged postoperative physiotherapy is performed. The surgical treatment for coronoid process hyperplasia is correction of the coronoid-malar interference by a coronoidectomy or simply coronoidotomy. Gerbino, et al., (1) reported that coronoidotomy was performed intraorally by an osteotomy at the base of the coronoid process in five patients and that this approach notably reduces the need for bone exposure and consequent surgical trauma compared to the coronoidectomy. With respect to postoperative physiotherapy, several devices are used for maintenance of sufficient interincisal distance. (1-3) Previously, a mouth-opening exerciser (HU-OS II) (4-6) was introduced for postoperative mouth-opening exercises in patients with severe trismus due to temporomandibular joint ankylosis after maxillectomy. The exerciser is available for increasing the mouth opening range without help postoperatively.
A case of unilateral coronoid hyperplasia is described that was successfully treated by coronoidotomy with prolonged postoperative physiotherapy, using a HU-OS II appliance and revealed the postoperative radiographic changes between the sectioned part of the coronoid process and the mandibular ascending ramus.
Case Report
A 28-year-old man was referred for evaluation of a persistent limited mouth opening. The patient first noticed the difficulty opening his mouth when he was 15 years old. He consulted a dentist and was given a diagnosis of temporomandibular joint disorder. There was no history of maxillofacial injury or familial occurrence of similar problems.
Clinical examination revealed limited mouth opening but no temporomandibular joint pain and no masticatory muscle tenderness. The maximum mouth opening was 30 mm. Left and right excursions were seven mm each and protrusive excursion was six mm. There was no dentofacial abnormality.
Orthopantomography showed the right coronid processes with normal length and the elongation of the left coronid processes (Figure 1). Computed tomography demonstrated the contact of the left zygomatic bone and the coronoid process in the open mouth position. Bone formation at the contact point on the posterior surface of the left zygomatic bone was observed (Figure 2 A-B). A diagnosis of left coronoid process hyperplasia was confirmed using the characteristic radiographic and clinical findings.
With the patient under general anesthesia, a coronoidotomy of the left coronoid process was performed intraorally by an osteotomy at the base of the coronoid process. A horizontal osteotomy was made with a Lindemann bur from the sigmoid incision to the anterior aspect of the ascending ramus (Figure 3A). The maximum mouth opening was 50 mm immediately after the osteotomy. The sectioned coronoid was not removed because there was no interference with enforced mandibular movement (Figure 3B).
Nine days after surgery, the maximum mouth opening was 33 mm. The patient started physiotherapy with a mouth-opening exerciser (HU-OS II) (Figure 4). The patient used the mouth-opening exerciser to do 100 consecutive openings using the exerciser with no other assistance--one opening per second, 100 seconds total. This exercise was done twice a day, once in the morning and once at night. Thirty days after surgery, the maximum mouth opening had increased to 40 mm, and at the three month follow-up, it had stabilized at 43 mm. The mechanical physiotherapy was then interrupted. At the 15 month follow-up, the maximum mouth opening range was still 43 mm, with good protrusion and lateral mandibular excursion, no displacement of the mandible, and no pain in the temporomandibular joint region.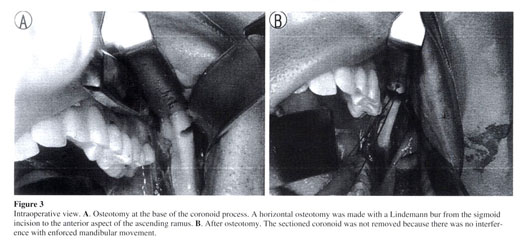
Radiographic follow-up showed that the coronoid process apparently united with the mandibular ascending ramus, with moderate dislocation and inclination posteriorly (Figures 5 and 6).
Discussion
The treatment of coronoid process hyperplasia, which presents essentially a mechanical problem, is primarily surgical. In a coronoidectomy, the ascending ramus of the mandible is exposed as far as the top of the coronoid process, and then the temporalis muscle is detached from the coronoid. The entire coronoid process is removed. Change in muscle activity with detachment of the temporalis muscle and postoperative fibrosis with removal of the coronoid may lead to displacement of the mandible and the other disappointing results. (1,2) However, Gerbino, et al., (1) described five patients with coronoid process hyperplasia, who were successfully treated by coronoidotomy, and reported that this approach notably reduces the need for bone exposure and consequent surgical trauma compared to the coronoidectomy. Furthermore, this technique without removal of the coronoid process also reduces the organization of a postsurgical hematoma, with consequential fibrosis at the site of the operation. In the current patient, a simple coronoidotomy was performed intraorally by an osteotomy at the base of the coronoid process. The favorable outcome of the coronoidotomy in this case may have been because there is less postsectioned fibrosis with this procedure and because the sectioned part of the coronoid can position itself and consolidated posteriorly.
The coronoid process heals onto the mandibular ascending ramus in such a posterior position that it does not cause further obstruct jaw movement. This may occur because it is pushed during mouth opening by the action of the temporal muscle during the early postoperative period, when the patient is most motivated to do the correct exercises. We introduced a mouth-opening exerciser (HU-OS II) (4-6) for postoperative mouth-opening exercises in the current patient. The exerciser is made of a five mm thick acrylic resin plate and is wedge-shaped with a cut tip. The exerciser has three mm long stairs so that patients can notice improvement in mouth-opening during exercise. Every stair has an extremely gentle slope so that it permits gradual mouth opening without severe pain. In previous reports, the management after coronoidotomy is not described in detail. (1,2) Tieghi, et al., (3) reported on two cases that received postoperative mouth opening exercises with a dynamic device (Darcissac type). The device was used for 10 hours per day for 30 days. In those two cases, three months after surgery, the maximum mouth opening increased to 40 mm. In the present case, 30 days after surgery, the maximum mouth opening had increased to 40 mm. HU-OS II is easy to use and very effective for postoperative mouth opening exercises.
In conclusion, in the present case, an intraoral coronoidotomy with postoperative physiotherapy for treatment of coronoid process hyperplasia allowed satisfactory and stable results in the correction of coronoid-malar interference.
References
(1.) Gerbino G, Bianchi SD, Bernardi M, Ben'one S: Hyperplasia of the mandibular coronoid process: long-term follow-up after coronoidotomy. J Craniomaxillofac Surg 1997; 25:169-173.
(2.) Shinno E, Sunakawa K, Hanasiro K, Shimoji M, Higa T: Anterior displacement of the mandible occurring after amputation of bilateral hyperplasia of the mandibular coronoid process. J Jpn Soc TMJ: 2002; 14:184-187.
(3.) Tieghi R, Galie M, Piersanti L, Clauser L: Bilateral hyperplasia of the coronoid processes: clinical report. J Craniofac Surg 2005; 16:723-726.
(4.) Murakami Y, Inoue N, Ahemed M, Yasuda M, Yamaguchi H, Totsuka Y: A new type of mouth-opening exerciser. Jpn J Oral Maxillofac Surg 1995; 41:175-177.
(5.) Murakami Y, Inoue N, Kobayashi T, Rin S, Ono M, Okada M, Saito S, Yamaguchi H, Nishikata S, Totsuka Y: Clinical study on postoperative physiotherapy in TMJ ankylosis. J Jpn Soc TMJ 1996; 8:105-117.
(6.) Inoue N, Murakami Y, Nishikata S, Oda M, Kobayashi T, Yamaguchi H, Saitoh S, Yura S, Yamaguchi T, Minowa K, Totsuka Y: Efficacy of post-operative physiotherapy in temporomandibular joint ankylosis. Hokkaido J Dent Sci 2000; 21:77-81.
Manuscript received August 14, 2007; revised manuscript received June 2, 2009; accepted June 4, 2009
Address for correspondence:
Dr. Shinya Yura
Dept. of Oral and Maxillofacial Surgery
Tonami General Hospital
1-61 Shintomi-cho, Tonami-city
Toyama-ken 939-1395
Japan
E-mail: yura@p1.coralnet.or.jp
Dr. Shinya Yura graduated from Hokkaido University School of Dentistry in 1987 and received his D.D.Sc. degree in 2002 at the same university. From 1995 to 2004, he served as an instructor and in 2004 as a lecturer in the Department of Oral and Maxillofacial Surgery at Hokkaido University School of Dentistry. Currently, Dr. Yura is a chief in the Department of Oral and Maxillofacial Surgery at Tonami General Hospital
Dr. Noritaka Ohga graduated from Hokkaido University School of Dentistry in 2001. From 2004 to 2005, he served as a resident in the Department of Oral and Maxillofacial Surgery at Tonami General Hospital.
Dr. Kazuhiro Ooi graduated from Hokkaido University School of Dentistry in 2000 and received his D.D.Sc. degree in 2005 at the same university. From 2005 to 2006, he served as a resident in the Department of Oral and Maxillofacial Surgery at Tonami General Hospital.
Dr. Yuri Izumiyama graduated from Hokkaido University School of Dentistry in 1999 and received his D.D.Sc. degree in 2004 at the same university. Currently, she is a resident in the Department of Oral and Maxillofacial Surgery at Tonami General.
Source Citation
Yura, Shinya, et al. "Mandibular coronoid hyperplasia: a case report." CRANIO: The Journal of Craniomandibular Practice 27.4 (2009): 275+. Gale Sciences Standard Package. Web. 13 May 2010.
Document URL
http://find.galegroup.com/gps/infomark.do?&contentSet=IAC-Documents&type=retrieve&tabID=T002&prodId=IPS&docId=A210722715&source=gale&srcprod=SP00&userGroupName=ptn045&version=1.0
Gale Document Number : A210722715
Rabu, 12 Mei 2010
Mandibular coronoid hyperplasia : a case report
Diposting oleh trinovrianti.physio di 22.35Effect of amitriptyline vs. physiotherapy in management of fibromyalgia syndrome : What predicts a clinical benefit ?
Diposting oleh trinovrianti.physio di 22.19Byline: M. Joshi, R. Joshi, A. Jain
Context : Fibromyalgia is a chronic disabling condition, and physicians treat it using a number of different treatment modalities. It is not known if one or more of such modalities are better than the others. We compared the efficacy of physiotherapy and amitriptyline in disability reduction in patients of fibromyalgia syndrome in a rural tertiary care hospital in Central India. Design : Open-label alternate patient treatment allocation. Materials and Methods : A six-month follow-up was done to assess the benefit of amitriptyline and physiotherapy for disability reduction in patients with fibromyalgia syndrome. Primary outcome measure was improvement in fibromyalgia impact questionnaire (FIQ) score. Statistical Analysis Used : Predictors of benefit were determined using multivariate logistic regression. Results : A total of 175 outpatients were assigned to either amitriptyline (n=87) or structured physiotherapy (n=88) treatments. There was a significant but similar (P=0.82) improvement in disability in both groups. High FIQ score at baseline and low socioeconomic status scores were significant predictors of benefit. Conclusions : Therapy with amitriptyline or physiotherapy is equally effective in improving outcome in patients of fibromyalgia over a period of six months.
Fibromyalgia syndrome is a non-articular rheumatic syndrome disorder comprising chronic widespread pain associated with variable symptoms.[sup] [1] It is a fairly common clinical entity, which is still poorly understood. Fibromyalgia is a major cause of morbidity and economic loss in the community and has a significant impact on patient's quality of life. Numerous studies assessing the resource utilization in rheumatic patients have found that patients of fibromyalgia have a multifold increased risk of lower wellbeing with a substantial cost burden.[sup] [2],[3],[4] The diagnosis of fibromyalgia is clinical, based on the American College of Rheumatology (ACR) criteria.[sup] [5] However, the pathogenesis, and clinical profile of fibromyalgia are poorly understood, and it frequently remains undiagnosed.[sup] [6]
A number of treatment options for fibromyalgia have been recommended, which include antidepressants, analgesics, exercise, cognitive behavioral therapy and other non-pharmacological interventions.[sup] [7],[8],[9] Of these options, antidepressants, analgesics and exercise have been studied in well-designed randomized control trials. Based on these trials, it has been found that there is a strong evidence favoring the use of amitryptiline and other tricyclic antidepressants.[sup] [10],[11] Recently, the US FDA has approved the use of pregabalin,[sup] [12] duloxetine[sup] [13] and milnacipran[sup] [14] for patients of fibromyalgia.[sup] [15] Exercise in the form of cardiovascular training, strength training, aerobics, flexibility training, all have led to improvement in patients of fibromyalgia.[sup] [10],[16]
Most of these studies have been done in the developed countries, and there is paucity of data about the burden of fibromyalgia, and performance of treatment options in developing countries. This is further complicated by the fact that most of the drugs advocated for treatment are expensive, need to be consumed for prolonged periods and hence are likely to be unaffordable in rural central India. Non-pharmacological modalities provide a reasonable alternative in this scenario. We conducted this study with an aim to compare the performance of physiotherapy and amitriptyline for disability reduction in patients with fibromyalgia. We also aimed to determine which clinical features at baseline would predict benefit with either therapy.
Materials and Methods
Setting The study was conducted at our institute, tertiary care hospital located in rural Central India. All outpatients presenting to the hospital are screened by doctors in general outpatient department (GOPD), where after a brief history and examination, appropriate referrals to specialists are advised. For the purpose of the study, doctors in GOPD were requested to advise patients with chronic muscular pain, of three months or greater in duration, to meet the study investigators.
Patients The investigators screened all patients who were referred to them for inclusion in the study. The inclusion criteria being age between 18 and 60 years, symptoms of chronic muscular pain of at least 12 weeks' duration, and fulfillment of ACR criteria (presence of tenderness in at least 11/18 trigger points) for the diagnosis of fibromyalgia syndrome (FMS).[sup] [5] Patients were excluded if they were pregnant or lactating, or had history of trauma, fractures, fever, malignancy, chronic renal or hepatic disorders, alcohol abuse, cerebrovascular or a neurological abnormality. Patients were allowed to continue their previous medications and exercise regimens, if any. The study was approved by the institutional ethics committee and participants were enrolled after obtaining a written informed consent.
Study procedures The patients included in the study were administered a standardized questionnaire to record socio-demographic characteristics, symptom characteristics and history of previous visits to a healthcare provider. The socioeconomic score (SES) was determined using a validated questionnaire. [sup][17] Briefly, the questionnaire consists of following: (1) household profile, (2) material possession profile, (3) educational profile, (4) occupational profile, (5) economic profile (6) possessed land or house cost profile and (7) social profile. Based on the average score in each of the above domains, SES was categorized into five grades: Grade 1: 57-70 points; Grade 2: 42-57 points; Grade 3: 27-42 points; Grade 4: 12- 27 points; and Grade 5: 0-12 points. Individuals in Grades 1 to 3 were considered as having a higher SES. Fibromyalgia impact questionnaire (FIQ) was used to determine a baseline score.[sup] [18] For the purpose of the study this questionnaire was translated into the local language (Marathi), and back-translated to English to ensure its accuracy. Minor modifications were done in the questionnaire to make it suitable for our setting (for example, the use of washer or dryer for laundry was modified to washing the laundry by themselves). Assessment of psychiatric co-morbidity was done using the Brief Psychiatric Rating Scale (BPRS), which is an 18-item instrument, with each item having seven severity grades.[sup] [19] A score of 32 or more indicates presence of psychopathology.[sup] [20]
The study investigator (MJ) was trained in the administration of these questionnaire-based instruments, and pilot tested them on a subset of patients before initiating the study. In addition erythrocyte sedimentation rate (ESR) and hemoglobin levels were obtained in all patients to determine the presence of anemia and collagen vascular diseases. We designed an open-label alternate patient treatment allocation strategy to observe and compare the performance of physiotherapy and amitriptyline in these patients. This observational study design was chosen as a pilot, and the study was open-labeled as it is difficult to conceal the treatments received. A trained physiotherapist conducted a uniform structured physical training and aerobic session for one group of patients. The patients were advised to perform the exercises daily twice for at least 10 min. There was a step-up pattern of exercise regimen followed by relaxation, stretching and strengthening techniques. The methodology is described in Box 1. The second group of patients received antidepressant in the form of open-label amitriptyline 25 mg once daily at bedtime. The dose of the drug was increased to 50 mg if no benefit was seen. No patient required further escalation of doses. All patients were also offered pharmacologic treatment with 50 mg tramadol in thrice daily doses and as required. The treatment recommendations were based on standard recommendations on the management of fibromyalgia.[sup] [10]
Follow-up All patients were followed up at monthly intervals for a period of six months. At each visit the study investigators determined the course of the disease and compliance with therapy. If patients adhered to [SUPPORTING:1] the prescribed therapies more than or equal to 2/3 days, they were considered to be compliant. The FIQ score was assessed at the end of the six monthly visits. Reduction in FIQ score from the baseline was used as the principle outcome measure.
Statistical analysis All data was double-entered using MS Excel. We performed a descriptive statistical analysis of the baseline data. The analyst (RJ) blinded to the treatment allocation compared the outcome measure (FIQ score at six months and reductions in FIQ score over six months) for the two groups using student's t -test (significance level 0.05). In the post hoc analysis we defined benefit as reduction in FIQ score of 2 standard deviations or more from the mean reduction over six months. We performed a univariate and a multivariate logistic regression to determine the demographic and clinical variables which predicted benefit. All statistical analysis was done using STATA version 9.0 (STATA Corp, College Road, Texas, USA).
Results
Between 1 March 2006 and 1 December 2007 a total of 324 patients were screened by the investigators and 175 (mean age: 38.8 6 9.3 with, 95% females) were included in the study. Amongst them, 19 patients (five in the amitriptyline group, and 14 in the physiotherapy group) were lost to follow-up and were not included in further analysis [Figure 1]. Hence the study sample consisted of 156 patients (82 in amitriptyline and 74 in physiotherapy groups).
Only one patient in the study fulfilled criteria for mild psychopathology, and the range of BPRS scores obtained was from 1 to 12. The range of ESR and hemoglobin levels was from 8 to 110 and 5.5 to 14, respectively. The baseline characteristics of the study patients in these two groups are described in [Table 1]. There was no statistically significant difference between the two groups in terms of baseline characteristics.
On follow-up, 65 (79.2%) patients in the amitriptyline group and 66 (89.2%) patients in the physiotherapy group reported adherence to the prescribed therapies for more than 75% days of the follow-up period. Of the 180 days of follow-up, the individuals in the amitriptyline and physiotherapy treatment groups adhered to treatment on an average for 135 (75%) and 141 (78%) days, respectively. Participants consumed narcotic analgesic (tramadol) on an average for 35 (19.4%) and 34 (18.8%) days in the amitriptyline and physiotherapy groups respectively; duration was similar in both groups. None of the patients had any major side-effects to warrant discontinuation of the therapy.
There was a significant improvement in the total FIQ scores at six months in both the treatment groups [Figure 2]. The mean reduction in FIQ score in both treatment groups being 12.37 (95% CI 10.71-14.04) in the amitriptyline group vs. 12.12 (95% CI 10.47-13.77) in the physiotherapy group ( P = 0.82). There was no difference in reduction of FIQ scores in the two groups.
The mean reduction in total FIQ score obtained in all patients combined was 12.2 [+ or -] SD 7.3 points. A total of 12 (14%) patients in the amitriptyline group, and seven (9%) patients in the physiotherapy group fulfilled the criteria for benefit (reduction in FIQ score by more than 22, which is more than 2 SD above mean). On multivariate analysis, patients who had a lower socioeconomic status and more disability (FIQ > 50) had significant benefit from either therapy [Table 2].
Discussion
The results of our study suggest that both amitriptyline and physiotherapy strategies significantly reduced disability due to fibromyalgia, as seen in a rural-based tertiary care hospital in central India. Both the strategies were equally effective in reduction of total FIQ score. Low socioeconomic status and high disability at baseline (as measured by FIQ score) were the only parameters that could predict benefit.
Our study has evaluated the effect of two different therapeutic modalities in the treatment of fibromyalgia. No similar study has been undertaken in the developing world. Our study had a few limitations, firstly a hierarchical screening method was used and this could have perhaps resulted in the small number of participants who were referred to the study investigator. As only clinical history was used for exclusion of patients, it could have potentially resulted in over-inclusion. However, in a resource-limited setting it was not feasible to perform laboratory investigations in all patients who were screened. Secondly, one-thirds of our study population was educated up to primary level only, and this could have limited the understanding of questionnaire-based scores. To overcome this we preferred interviewed questionnaire rather than using a self-administered questionnaire. Thirdly, given the nature of interventions, allocation could not be concealed. Lack of allocation concealment raises a high risk of bias. As fibromyalgia is a chronic illness it is likely that study duration was not long enough to demonstrate any significant benefit. The improvement in both the groups could be linked to Hawthorn effect or regression towards the mean. It does not mean that both treatments are effective. This could be a major limitation.
There could be a possibility that the improvement observed in both the groups could, to some extent, be attributed to the use of tramadol. Keeping a control group receiving only tramadol could have helped to assess this possibility. Lastly, the rate of loss to follow-up was relatively important and patients lost to follow-up were excluded in the statistical analyses. Despite tracing them to their residential addresses we could not obtain cooperation and decided to exclude them from the final analysis.
We did not find any co-morbid psychiatric illness based on the questionnaire used. It is likely that we underestimated the prevalence of depression, anxiety which are common associations of the disease. There could have been cultural issues which could have prevented expression of psycho-social concerns. Future studies are required to bring out the psychiatric associations in these patients.
We reviewed similar studies which were done in past to compare the effects of amitriptyline and physiotherapy. We found that a study evaluating the combined benefit of amitriptyline and exercise[sup] [21] showed that only the combination of amitriptyline and exercise had significant improvements at three months.[sup] [21] Recently, Salek et al. found no significant differences between exercise and anti-depressant group vs. amitriptyline only groups in a randomized trial.[sup] [22] None of the studies have evaluated predictors which explain benefit.
Our study indicates that amitriptyline and physiotherapy are equally beneficial in patients of fibromyalgia. Our study is also unique in the respect that we have studied factors which could help to predict response to either therapy. We found that patients with low socioeconomic scale had better response to therapy. This could be due to the fact that these patients have poor access to health facility and feel psychologically better on receiving care. We also found that patients with high disability score had better outcomes, probably due to higher quantum of relief expected.
We conclude that amitriptyline and physiotherapy are equally beneficial in improving outcome in patients of fibromyalgia, as seen in the study population in a rural-based tertiary care hospital in central India. Considering the cost of drug therapy we recommend use of physiotherapy over amitriptyline in resource-limited settings.
References
1. Mease P. Fibromyalgia syndrome: Review of clinical presentation, pathogenesis, outcome measures and treatment. J Rheumatol Suppl 2005;75:6-21.
2. Boonen A, van den Heuvel R, van Tubergen A, Goossens M, Severens JL, van der Heijde D, et al. Large differences in cost of illness and wellbeing between patients with fibromyalgia, chronic low back pain, or ankylosing spondylitis. Ann Rheum Dis 2005;64:396-402.
3. Sicras-Mainar A, Rejas J, Navarro R, Blanca M, Morcillo A, Larios R, et al. Treating patients with fibromyalgia in primary care settings under routine medical practice: A claim database cost and burden of illness study. Arthritis Res Ther 2009;11:R54.
4. Spaeth M. Epidemiology, costs, and the economic burden of fibromyalgia. Arthritis Res Ther 2009;11:117.
5. Wolfe F, Smythe HA, Yunus MB, Bennett RM, Bombardier C, Goldenberg DL, et al. The American College of Rheumatology 1990 criteria for the classification of fibromyalgia. Arthritis Rheum 1990;33:160-72.
6. Lakomek HJ, Lakomek M, Bosquet-Nahrwold K. Fibromyalgia Diagnostics-disease approach-therapy. Med Klin (Munich) 2007;102:23-9.
7. Staud R. Treatment of fibromyalgia and its symptoms. Expert Opin Pharmacother 2007;8:1629-42.
8. Arnold LM. Biology and therapy of fibromyalgia: New therapies in fibromyalgia. Arthritis Res Ther 2006;8:212.
9. Harris RE, Clauw DJ. Newer treatments for fibromyalgia syndrome. Ther Clin Risk Manag 2008;4:1331-42.
10. Goldenberg DL, Burckhardt C, Crofford L. Management of Fibromyalgia Syndrome. JAMA 2004;292:2388-95.
11. Hauser W, Bernardy K, U?eyler N, Sommer C. Treatment of fibromyalgia syndrome with antidepressants: A meta-analysis. JAMA 2009;301:198-209.
12. Ablin JN, Buskila D. Emerging therapies for fibromyalgia. Expert Opin Emerg Drugs 2008;13:53-62.
13. Yan J. Antidepressant Gets FDA Nod to Treat Fibromyalgia. Psychiatr News 2008;43:6. Available from: http://pn.psychiatryonline.org/cgi/content/full/43/14/6 . [accessed on 2009 Aug 12].
14. Mease PJ, Clauw DJ, Gendreau RM, Rao SG, Kranzler J, Chen W, et al. The efficacy and safety of milnacipran for treatment of fibromyalgia:A randomized, double-blind, placebo-controlled trial. J Rheumatol 2009;36:398-409.
15. Kim L, Lipton S, Deodhar A. Pregabalin for fibromyalgia: Some relief but no cure. Cleve Clin J Med 2009;76:255-61.
16. Busch AJ, Barber KA, Overend TJ, Peloso PM, Schachter CL. Exercise for treating fibromyalgia syndrome. Cochrane Database Syst Rev 2007;4:CD003786.
17. Tiwari SC, Kumar A, Kumar A. Development and standardization of a scale to measure socio-economic status in urban and rural communities in India. Indian J Med Res 2005;122:309-14.
18. Bennett R. The Fibromyalgia Impact Questionnaire (FIQ): A review of its development, current version, operating characteristics and uses. Clin Exp Rheumatol 2005;23:S154-62.
19. Pull CB, Overall JE. Adequacy of the Brief Psychiatric Rating Scale for distinguishing lesser forms of psychopathology. Psychol Rep 1977;40:167-73.
20. Leucht S, Kane JM, Kissling W, Hamann J, Etschel E, Engel R. Clinical implications of Brief Psychiatric Rating Scale scores. Br J Psychiatry 2005;187:366-71.
21. Isomeri R, Mikkelsson M, Latikka P, Kammonen K. Effects of amitriptyline and cardiovascular fitness training on pain in patients with primary fibromyalgia. J Musculoskelet Pain 1993;1:253-60.
22. Salek AK, Khan MM, Ahmed SM, Rashid MI, Emran MA, Mamun MA. et al. Effect of aerobic exercise on patients with primary fibromyalgia syndrome. Mymensingh Med J 2005;14:141-4.
Source Citation
Joshi, M., R. Joshi, and A. Jain. "Effect of amitriptyline vs. physiotherapy in management of fibromyalgia syndrome: What predicts a clinical benefit?." Journal of Postgraduate Medicine July-Sept. 2009: 185. CPSN. Web. 13 May 2010.
Document URL
http://find.galegroup.com/gps/infomark.do?&contentSet=IAC-Documents&type=retrieve&tabID=T002&prodId=IPS&docId=A211206622&source=gale&srcprod=CPSN&userGroupName=ptn045&version=1.0
Gale Document Number:A211206622