




ABSTRACT
A case of unilateral coronoid hyperplasia successfully treated by corenoidotomy with prolonged postoperative physiotherapy and reveal the postoperative radiographic changes between the sectioned part of the coronoid process and the mandibular ascending ramus is described. The patient was a 28-year-old man whose maximum mouth opening was 30 mm. A coronoidotomy of the left coronoid process was performed. Nine days after surgery, the patient started physiotherapy with a HU-OSr appliance. After coronoidotomy and physiotherapy, the maximum mouth opening had increased to 43 mm. Radiographic follow-up showed that the coronoid process apparently united with the mandibular ascending ramus, with moderate dislocation and inclination posteriorly. In the case presented, an intraoral coronoidotomy with postoperative physiotherapy for treatment of coronoid process hyperplasia allowed satisfactory and stable results in the correction of coronoid-malar interference.
**********
In patients with coronoid process hyperplasia, which presents essentially a mechanical problem such as limited mouth opening, a surgical treatment with prolonged postoperative physiotherapy is performed. The surgical treatment for coronoid process hyperplasia is correction of the coronoid-malar interference by a coronoidectomy or simply coronoidotomy. Gerbino, et al., (1) reported that coronoidotomy was performed intraorally by an osteotomy at the base of the coronoid process in five patients and that this approach notably reduces the need for bone exposure and consequent surgical trauma compared to the coronoidectomy. With respect to postoperative physiotherapy, several devices are used for maintenance of sufficient interincisal distance. (1-3) Previously, a mouth-opening exerciser (HU-OS II) (4-6) was introduced for postoperative mouth-opening exercises in patients with severe trismus due to temporomandibular joint ankylosis after maxillectomy. The exerciser is available for increasing the mouth opening range without help postoperatively.
A case of unilateral coronoid hyperplasia is described that was successfully treated by coronoidotomy with prolonged postoperative physiotherapy, using a HU-OS II appliance and revealed the postoperative radiographic changes between the sectioned part of the coronoid process and the mandibular ascending ramus.
Case Report
A 28-year-old man was referred for evaluation of a persistent limited mouth opening. The patient first noticed the difficulty opening his mouth when he was 15 years old. He consulted a dentist and was given a diagnosis of temporomandibular joint disorder. There was no history of maxillofacial injury or familial occurrence of similar problems.
Clinical examination revealed limited mouth opening but no temporomandibular joint pain and no masticatory muscle tenderness. The maximum mouth opening was 30 mm. Left and right excursions were seven mm each and protrusive excursion was six mm. There was no dentofacial abnormality.
Orthopantomography showed the right coronid processes with normal length and the elongation of the left coronid processes (Figure 1). Computed tomography demonstrated the contact of the left zygomatic bone and the coronoid process in the open mouth position. Bone formation at the contact point on the posterior surface of the left zygomatic bone was observed (Figure 2 A-B). A diagnosis of left coronoid process hyperplasia was confirmed using the characteristic radiographic and clinical findings.
With the patient under general anesthesia, a coronoidotomy of the left coronoid process was performed intraorally by an osteotomy at the base of the coronoid process. A horizontal osteotomy was made with a Lindemann bur from the sigmoid incision to the anterior aspect of the ascending ramus (Figure 3A). The maximum mouth opening was 50 mm immediately after the osteotomy. The sectioned coronoid was not removed because there was no interference with enforced mandibular movement (Figure 3B).
Nine days after surgery, the maximum mouth opening was 33 mm. The patient started physiotherapy with a mouth-opening exerciser (HU-OS II) (Figure 4). The patient used the mouth-opening exerciser to do 100 consecutive openings using the exerciser with no other assistance--one opening per second, 100 seconds total. This exercise was done twice a day, once in the morning and once at night. Thirty days after surgery, the maximum mouth opening had increased to 40 mm, and at the three month follow-up, it had stabilized at 43 mm. The mechanical physiotherapy was then interrupted. At the 15 month follow-up, the maximum mouth opening range was still 43 mm, with good protrusion and lateral mandibular excursion, no displacement of the mandible, and no pain in the temporomandibular joint region.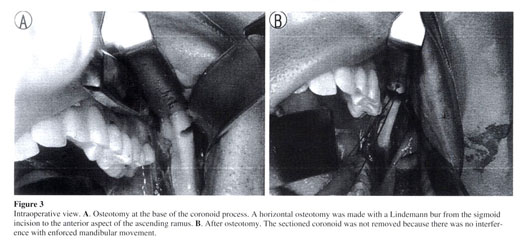
Radiographic follow-up showed that the coronoid process apparently united with the mandibular ascending ramus, with moderate dislocation and inclination posteriorly (Figures 5 and 6).
Discussion
The treatment of coronoid process hyperplasia, which presents essentially a mechanical problem, is primarily surgical. In a coronoidectomy, the ascending ramus of the mandible is exposed as far as the top of the coronoid process, and then the temporalis muscle is detached from the coronoid. The entire coronoid process is removed. Change in muscle activity with detachment of the temporalis muscle and postoperative fibrosis with removal of the coronoid may lead to displacement of the mandible and the other disappointing results. (1,2) However, Gerbino, et al., (1) described five patients with coronoid process hyperplasia, who were successfully treated by coronoidotomy, and reported that this approach notably reduces the need for bone exposure and consequent surgical trauma compared to the coronoidectomy. Furthermore, this technique without removal of the coronoid process also reduces the organization of a postsurgical hematoma, with consequential fibrosis at the site of the operation. In the current patient, a simple coronoidotomy was performed intraorally by an osteotomy at the base of the coronoid process. The favorable outcome of the coronoidotomy in this case may have been because there is less postsectioned fibrosis with this procedure and because the sectioned part of the coronoid can position itself and consolidated posteriorly.
The coronoid process heals onto the mandibular ascending ramus in such a posterior position that it does not cause further obstruct jaw movement. This may occur because it is pushed during mouth opening by the action of the temporal muscle during the early postoperative period, when the patient is most motivated to do the correct exercises. We introduced a mouth-opening exerciser (HU-OS II) (4-6) for postoperative mouth-opening exercises in the current patient. The exerciser is made of a five mm thick acrylic resin plate and is wedge-shaped with a cut tip. The exerciser has three mm long stairs so that patients can notice improvement in mouth-opening during exercise. Every stair has an extremely gentle slope so that it permits gradual mouth opening without severe pain. In previous reports, the management after coronoidotomy is not described in detail. (1,2) Tieghi, et al., (3) reported on two cases that received postoperative mouth opening exercises with a dynamic device (Darcissac type). The device was used for 10 hours per day for 30 days. In those two cases, three months after surgery, the maximum mouth opening increased to 40 mm. In the present case, 30 days after surgery, the maximum mouth opening had increased to 40 mm. HU-OS II is easy to use and very effective for postoperative mouth opening exercises.
In conclusion, in the present case, an intraoral coronoidotomy with postoperative physiotherapy for treatment of coronoid process hyperplasia allowed satisfactory and stable results in the correction of coronoid-malar interference.
References
(1.) Gerbino G, Bianchi SD, Bernardi M, Ben'one S: Hyperplasia of the mandibular coronoid process: long-term follow-up after coronoidotomy. J Craniomaxillofac Surg 1997; 25:169-173.
(2.) Shinno E, Sunakawa K, Hanasiro K, Shimoji M, Higa T: Anterior displacement of the mandible occurring after amputation of bilateral hyperplasia of the mandibular coronoid process. J Jpn Soc TMJ: 2002; 14:184-187.
(3.) Tieghi R, Galie M, Piersanti L, Clauser L: Bilateral hyperplasia of the coronoid processes: clinical report. J Craniofac Surg 2005; 16:723-726.
(4.) Murakami Y, Inoue N, Ahemed M, Yasuda M, Yamaguchi H, Totsuka Y: A new type of mouth-opening exerciser. Jpn J Oral Maxillofac Surg 1995; 41:175-177.
(5.) Murakami Y, Inoue N, Kobayashi T, Rin S, Ono M, Okada M, Saito S, Yamaguchi H, Nishikata S, Totsuka Y: Clinical study on postoperative physiotherapy in TMJ ankylosis. J Jpn Soc TMJ 1996; 8:105-117.
(6.) Inoue N, Murakami Y, Nishikata S, Oda M, Kobayashi T, Yamaguchi H, Saitoh S, Yura S, Yamaguchi T, Minowa K, Totsuka Y: Efficacy of post-operative physiotherapy in temporomandibular joint ankylosis. Hokkaido J Dent Sci 2000; 21:77-81.
Manuscript received August 14, 2007; revised manuscript received June 2, 2009; accepted June 4, 2009
Address for correspondence:
Dr. Shinya Yura
Dept. of Oral and Maxillofacial Surgery
Tonami General Hospital
1-61 Shintomi-cho, Tonami-city
Toyama-ken 939-1395
Japan
E-mail: yura@p1.coralnet.or.jp
Dr. Shinya Yura graduated from Hokkaido University School of Dentistry in 1987 and received his D.D.Sc. degree in 2002 at the same university. From 1995 to 2004, he served as an instructor and in 2004 as a lecturer in the Department of Oral and Maxillofacial Surgery at Hokkaido University School of Dentistry. Currently, Dr. Yura is a chief in the Department of Oral and Maxillofacial Surgery at Tonami General Hospital
Dr. Noritaka Ohga graduated from Hokkaido University School of Dentistry in 2001. From 2004 to 2005, he served as a resident in the Department of Oral and Maxillofacial Surgery at Tonami General Hospital.
Dr. Kazuhiro Ooi graduated from Hokkaido University School of Dentistry in 2000 and received his D.D.Sc. degree in 2005 at the same university. From 2005 to 2006, he served as a resident in the Department of Oral and Maxillofacial Surgery at Tonami General Hospital.
Dr. Yuri Izumiyama graduated from Hokkaido University School of Dentistry in 1999 and received his D.D.Sc. degree in 2004 at the same university. Currently, she is a resident in the Department of Oral and Maxillofacial Surgery at Tonami General.
Source Citation
Yura, Shinya, et al. "Mandibular coronoid hyperplasia: a case report." CRANIO: The Journal of Craniomandibular Practice 27.4 (2009): 275+. Gale Sciences Standard Package. Web. 13 May 2010.
Document URL
http://find.galegroup.com/gps/infomark.do?&contentSet=IAC-Documents&type=retrieve&tabID=T002&prodId=IPS&docId=A210722715&source=gale&srcprod=SP00&userGroupName=ptn045&version=1.0
Gale Document Number : A210722715
Rabu, 12 Mei 2010
Mandibular coronoid hyperplasia : a case report
Diposting oleh trinovrianti.physio di 22.35
Subscribe to:
Posting Komentar (Atom)
0 komentar:
Posting Komentar